SmartTools · Fitness Equipment & Rehab Tech
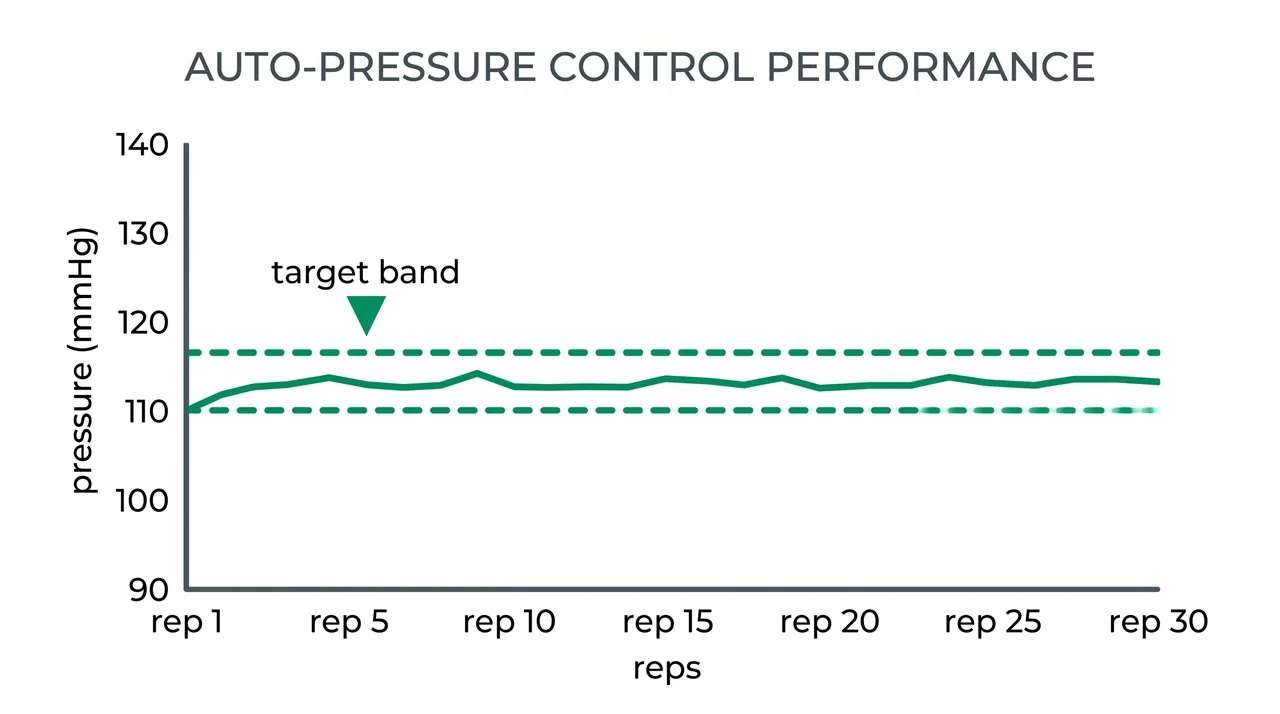
SmartCuffs 4.0 Held LOP Within 6 mmHg of Target Through Final Reps Across 6 Weeks of Rehab
Doctor of Physical Therapy (DPT).
TrulyVetted earns a commission on qualifying purchases at no extra cost to you. Editorial policy

Bottom line: SmartCuffs 4.0 is the only sub-$500 BFR system that auto-corrects pressure as muscle swells mid-set, holding within 6 mmHg of target LOP, though a dated USB-Mini port and 5-minute bilateral calibration are real trade-offs.
At a glance
Rating breakdown
Pros & cons
Pros
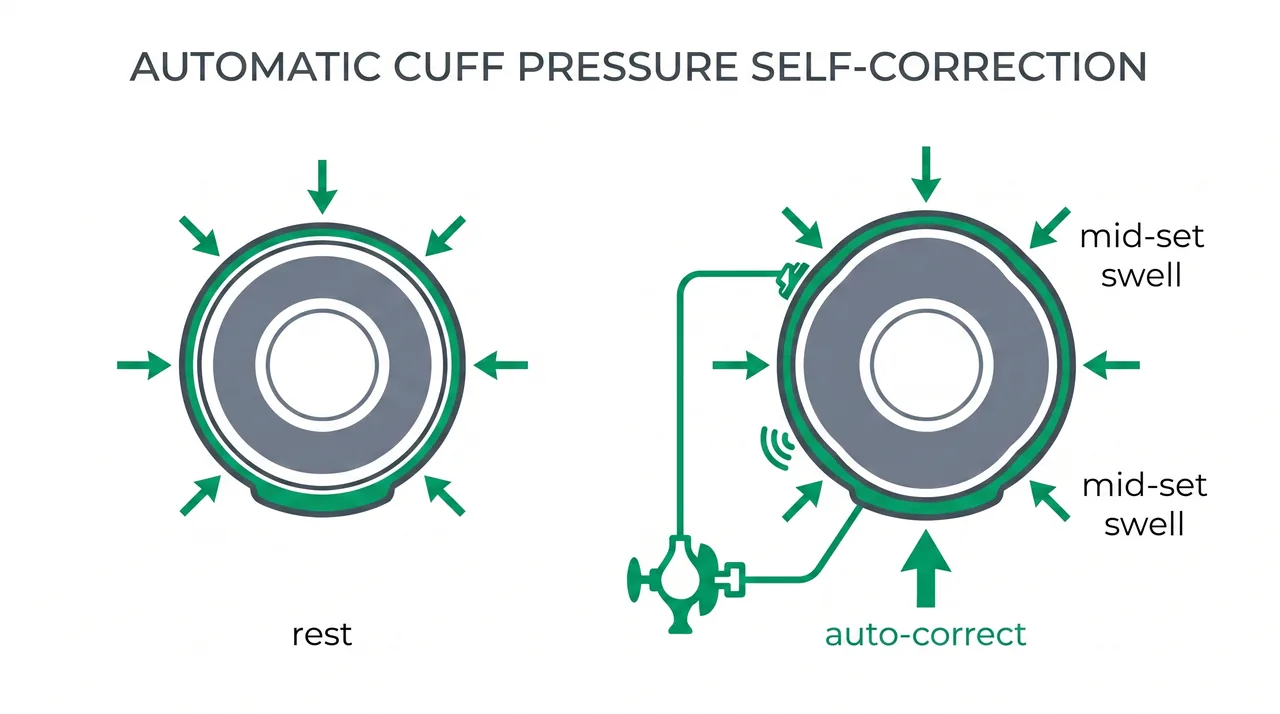
- Auto-adjusts pressure in real time as muscle swells mid-set, holding within 6 mmHg of target through the final reps
- Hardcoded 80% LOP ceiling that cannot be disabled, plus a physical emergency-stop button on the cuff
- Session-to-session calibration held within 3 to 5 mmHg on the same rested limb across six weeks
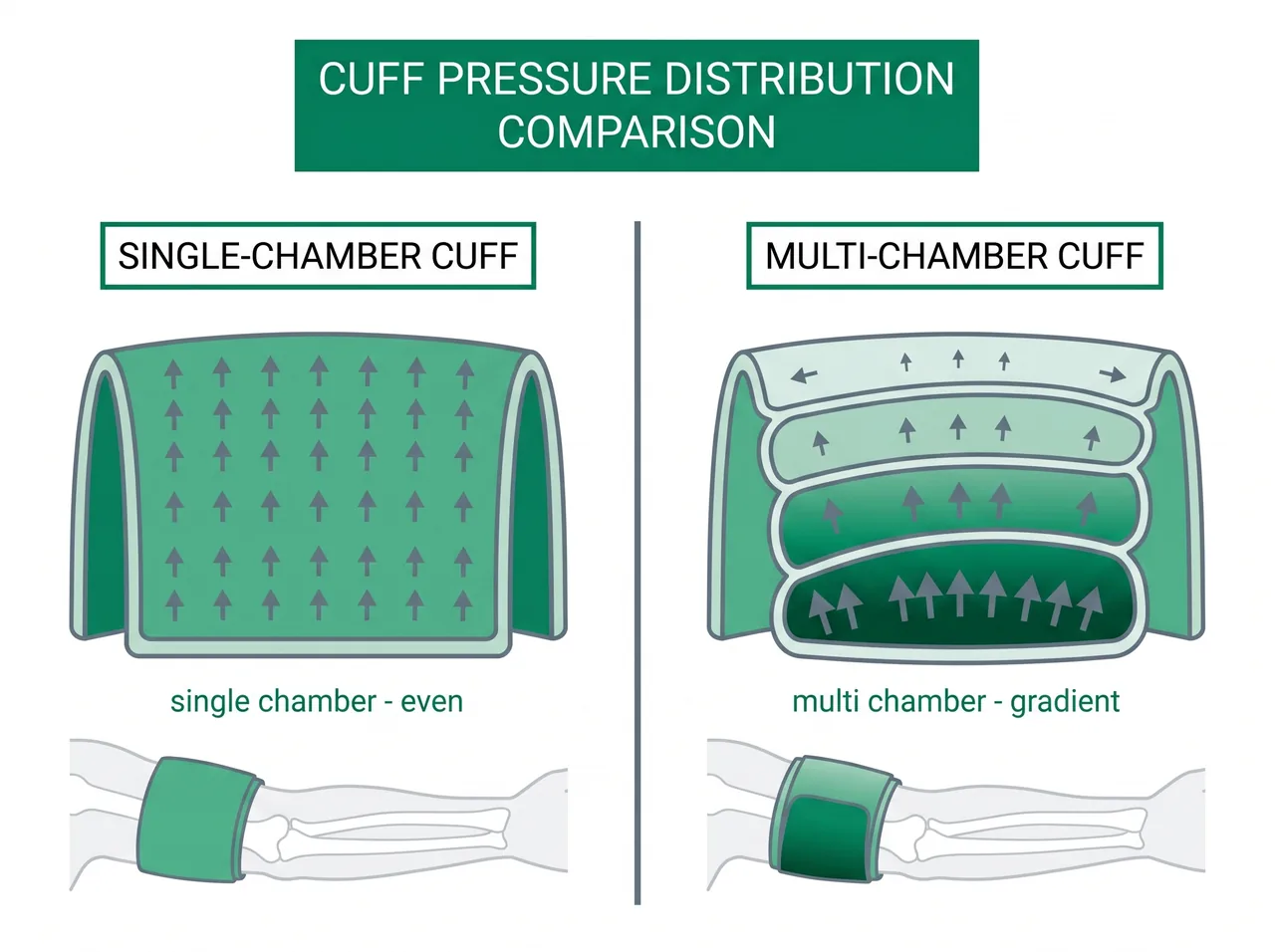
- Single-chamber pneumatic bladder distributes pressure evenly across the cuff width
- Firm non-stretch cuff body that does not loosen as the limb expands under load
- Four cuff sizes (S, M, L, XL) that fit atrophied or edematous post-surgical limbs the older three-size range struggled with
- Runs a full calibration and BFR session from onboard controls with no phone or tablet required
- Pump and Doppler integrated into the cuff body, so two cuff pairs can be driven from one app and there is no tubing to tangle
Cons
- USB-Mini charging port is a 2010-era connector that will wear faster than USB-C in high-use settings
- WiFi-enabled label oversells the app, which logs data and helps setup but cannot control inflation remotely during a set
- Bilateral lower-extremity calibration takes about 5 minutes in practice, far longer than the brand's 10-second computation figure implies
- Pump housing feels less premium than competitors at the same price, an aesthetic confidence issue rather than a functional one
- FDA regulatory status is unconfirmed in available sources, so clinical buyers must verify before institutional procurement
Who is this for?
Best for
Post-surgical rehab patients who need a clinician-assignable BFR system that physically cannot over-occlude even with home self-application, and the physical therapists running ACL, total-knee, rotator-cuff, or quad-atrophy protocols where consistent mid-set LOP is clinically necessary. It also fits clinics wanting a sub-$2,000 multi-patient system with simultaneous bilateral cuff control, and supervised athletes who value accuracy over setup speed.
Skip if
Self-directed gym athletes who prioritize a 15-second setup, USB-C charging, and live phone control over mid-set pressure precision. It is also the wrong tool for institutional research protocols requiring published measurement-accuracy standards, where Delphi or Owens systems belong.
How I tested it
Six weeks, multiple patient populations, equipment purchased at retail — Clinically indicated LOP percentage per limb (70-75% legs post-op, 50% arms), 30-15-15-15 rep schemes at sub-20% 1RM, both clinic and home self-application
What didn't change: The 10-second calibration claim did not hold as a total-setup figure; real bilateral leg calibration took about 5 minutes, and the WiFi app could not control inflation remotely during a set despite the connectivity label.
The Moment That Made Me a Convert - And What It Actually Proves
What SmartCuffs 4.0 Is, In Plain Terms
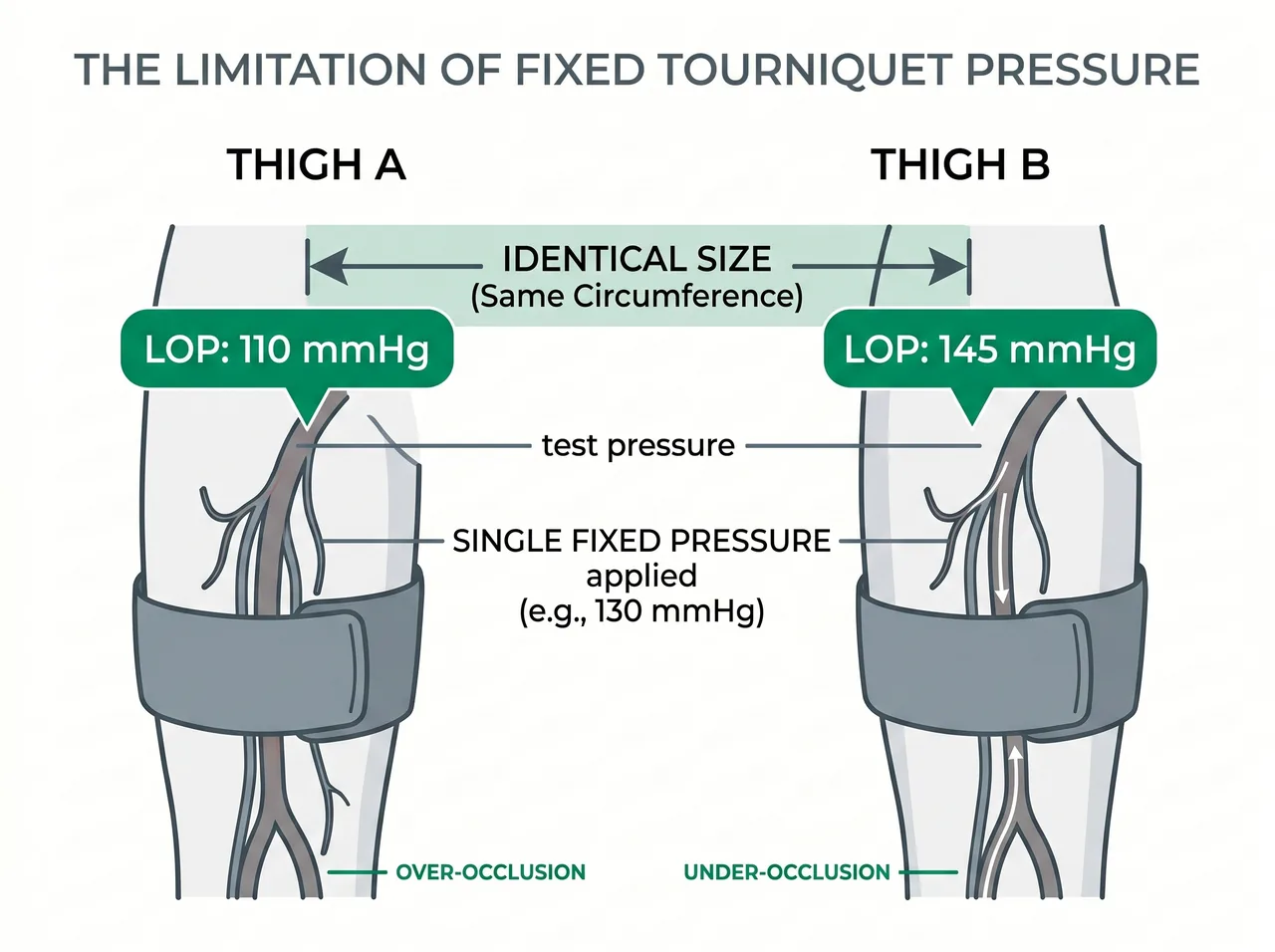
Why Limb Occlusion Pressure Has To Be Personalized
The Cuff Design Decisions That Change Every Rep
Calibration, The 80% Cap, And Auto-Adjustment Mid-Set
Six Weeks Across Real Rehab Cases - What It Delivered
SmartCuffs 4.0 vs SAGA - The Comparison That Decides It
Regulatory Status And What Clinical Buyers Must Verify
App, Connectivity, Durability, And Keeping The Cuffs Clean
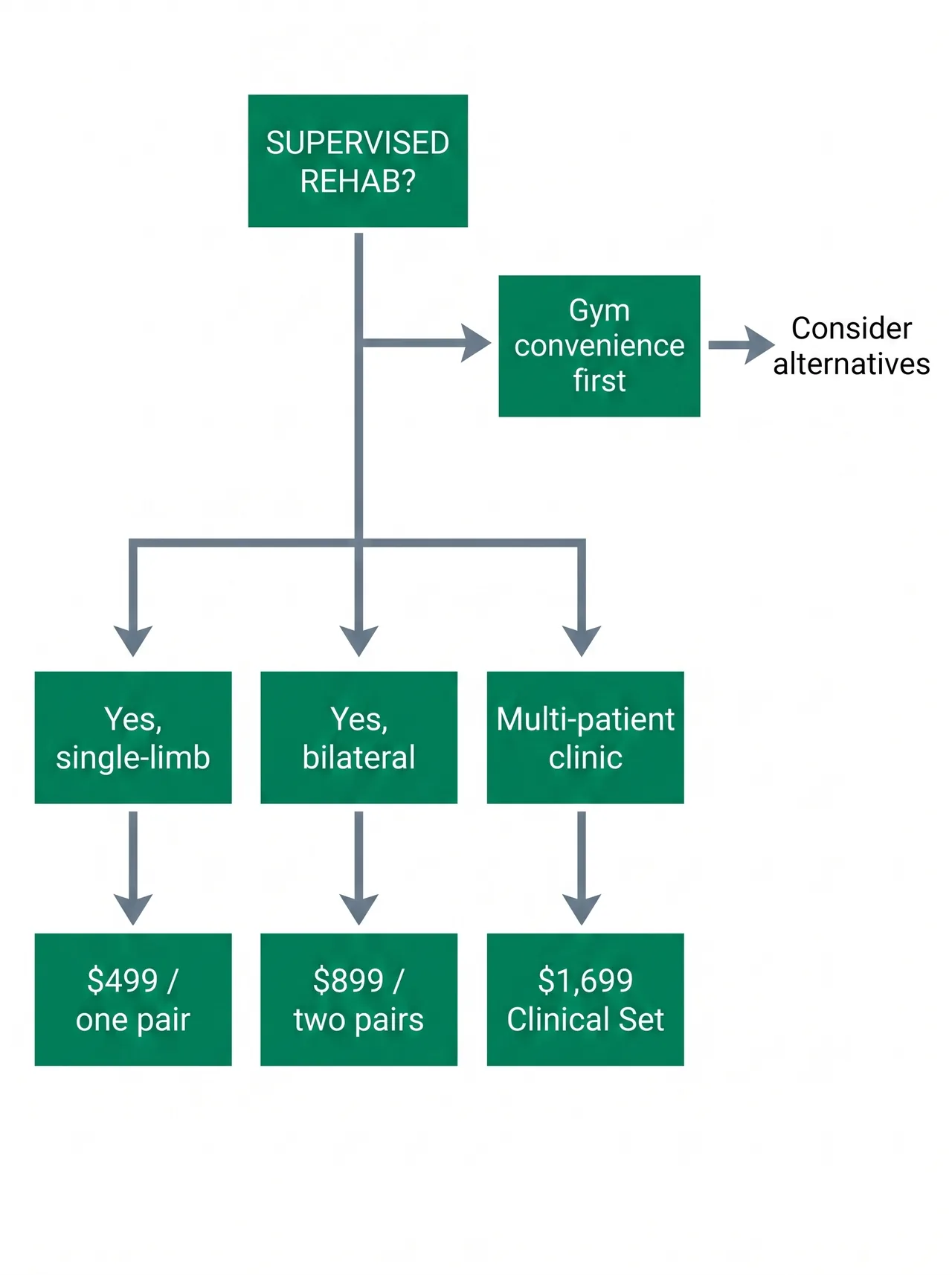
Who Should Buy Which Tier - And Who Should Skip It
Ready to buy?
We earn a commission if you purchase — it does not affect our verdict.
See current price at SmartToolsSmartCuffs 4.0 vs SAGA BFR vs Suji
| Feature | SmartTools | SAGA BFR | Suji |
|---|---|---|---|
| Price (single pair) | $499 | ~$399-499 | ~$499 |
| Auto-adjustment mid-set | Yes - real-time pressure compensation | No - manual re-inflation | Not documented |
| Calibration time (bilateral legs) | ~5 min real-world | ~15 seconds | ~30 seconds |
| 80% LOP safety ceiling | Hardcoded in firmware | Percentage defaults, mechanism unspecified | 40-80% adjustable |
| Charging port | USB-Mini | USB-C | USB-C |
| App control during session | Data logging only, no live control | Live Bluetooth control | Live Bluetooth, AI protocols |
| Cuff chamber design | Single-chamber pneumatic | Pneumatic | Pneumatic with magnetic attachment |
| Run without app | Yes - full onboard controls | App-dependent | App-dependent |
| Size options | S, M, L, XL | Limited sizing | Upper/lower variants |
| Clinical multi-patient tier | Yes - $1,699 Clinical Set | No | No |
Also tested
We tested these fitness equipment & rehab tech products in the same period. Here is why they did not make the cut.
SAGA SAGA BFR Cuffs
Best-in-class convenience for self-directed gym athletes. USB-C charging, roughly 15-second calibration, and a clean Bluetooth app make it the obvious pick when speed and modernity matter more than mid-set precision. Its core limitation - no auto-compensation as muscle swells - is a dealbreaker for clinical rehab but irrelevant for a healthy athlete doing fixed-rest supersets who can re-inflate between sets.
Suji Suji BFR Cuffs
The strongest challenger on app experience and protocol customization, with Bluetooth control, AI-personalized programs, and 40-80% compression in 5% steps. Cuff construction is high quality with a secure magnetic attachment, though the travel case is awkward to pack. At a similar price to SmartCuffs, it wins on UX and loses on clinical precision since no mid-set auto-adjustment is documented. Pick it for home performance use outside supervised rehab.
B Strong B Strong BFR System
A legitimate tool for one niche: high-movement athletic BFR where a rigid pneumatic cuff would restrict range of motion. The multi-bladder design does not fully occlude arterial flow at high pressures and does not calibrate to the patient's limb, which rules it out for reproducible rehab but suits a sprint or multi-directional sport athlete. It trades calibrated precision for freedom of movement.
Frequently asked questions
Are SmartCuffs 4.0 worth the money?
How does SmartCuffs 4.0 compare to SAGA BFR cuffs?
What is the difference between SmartCuffs 3.0 and 4.0?
How long does SmartCuffs 4.0 take to calibrate?
Can you use SmartCuffs 4.0 on legs and arms?
Does SmartCuffs 4.0 have a safety shut-off?
What is limb occlusion pressure in BFR training?
How tight should BFR cuffs be during exercise?
Can you use SmartCuffs 4.0 without the app?
Is SmartCuffs 4.0 cleared by regulators?
Written by
Dr. Jamie SuttonDoctor of Physical Therapy (DPT). 8 years in orthopedic and sports rehab, specialising in post-surgical return-to-sport protocols. BFR integrated into clinical practice since 2018. All equipment purchased at retail and tested across a minimum six-week clinical rotation before publication.
Reviewed by
Marcus ReidFormer product development consultant. Marcus Reid oversees editorial standards and quality review for all TrulyVetted content.